What is L-DOPA used for?
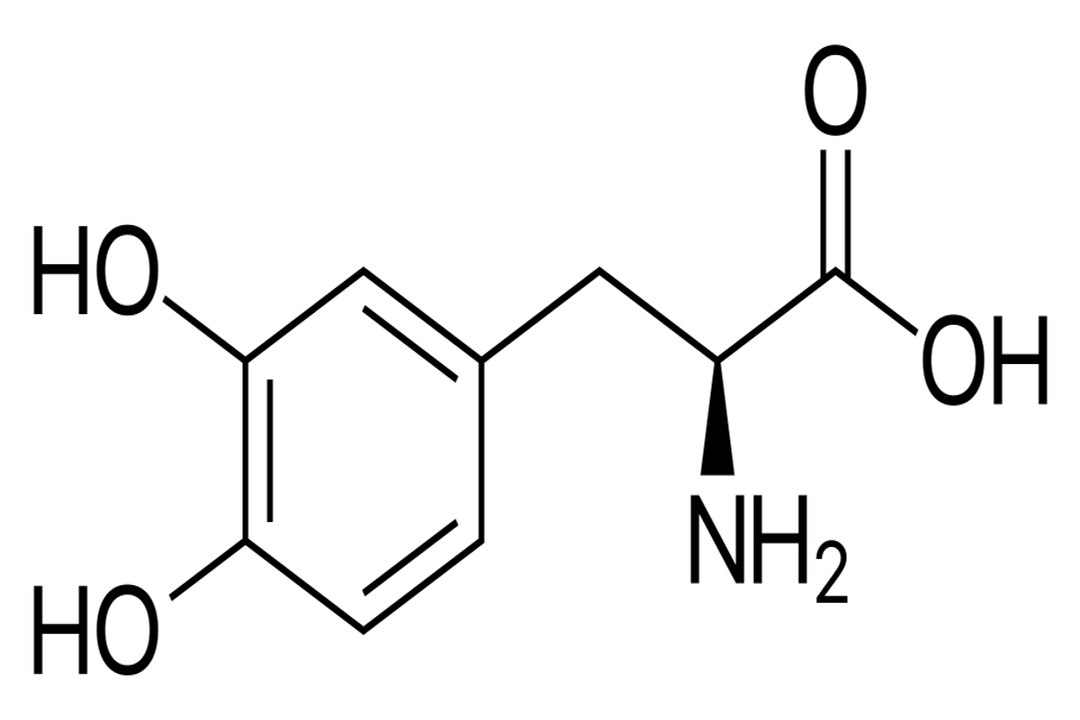
L-DOPA, short for Levodopa, is fundamentally known as the primary treatment for managing the symptoms of Parkinson’s disease. [6][9] To understand its significance, one must first understand its relationship with dopamine. Dopamine is a critical neurotransmitter in the brain that plays many roles, including regulating movement. [6] In Parkinson's disease, the cells responsible for producing dopamine in the brain begin to degenerate, leading to a deficit of this essential chemical. [6][9] When dopamine levels drop too low, people experience the hallmark physical symptoms of the condition, such as tremors, muscle stiffness, and slowness of movement. [6][9]
# Precursor Mechanism
L-DOPA itself is not dopamine, but rather its direct chemical precursor. [1][5] This distinction is medically vital because dopamine, when taken orally, cannot effectively cross the blood-brain barrier (BBB), the protective shield that separates the circulating blood from the central nervous system. [1][5][6] If dopamine cannot enter the brain, it cannot correct the deficit causing the motor symptoms. L-DOPA, however, is designed to pass through the BBB relatively unimpeded. [5] Once inside the brain tissue, specific enzymes convert the L-DOPA into usable dopamine, effectively replenishing the depleted supply. [1][5] This process allows clinicians to restore some level of dopamine function, providing symptomatic relief where simply administering dopamine could not. [6]
# Parkinson's Treatment
The introduction of L-DOPA revolutionized the treatment landscape for Parkinson’s disease decades ago, offering functional improvement where treatments were previously minimal. [6][10] It remains the most effective medication available for controlling the motor symptoms associated with the condition. [9] By increasing the amount of dopamine available in the brain, L-DOPA helps patients regain control over voluntary movements, making actions like walking, speaking, and simple daily tasks much more manageable. [6]
While L-DOPA addresses the motor deficits, it is important to recognize that it does not halt the progression of the underlying disease itself, which is a neurodegenerative disorder. [10] It acts as a powerful symptomatic treatment, managing the effects of the dopamine loss rather than curing the cause of the cell death. [6][10]

# Combination Necessity
When L-DOPA is administered alone, the body has mechanisms to convert a significant portion of it into dopamine before it ever reaches the brain, specifically in the peripheral systems like the bloodstream and other organs. [4][7] This premature conversion causes several problems. First, it wastes the drug, meaning less active ingredient makes it to the target site. Second, this peripheral dopamine causes very unpleasant side effects, most notably severe nausea and vomiting. [4][7]
To counteract this peripheral conversion, L-DOPA is almost always prescribed alongside a second medication, most commonly Carbidopa. [4][6][7] Carbidopa functions as an inhibitor of the enzyme DOPA decarboxylase in the periphery. [4] By inhibiting this enzyme outside the brain, Carbidopa effectively shields the L-DOPA from premature breakdown. This allows a much higher percentage of the oral dose to cross the BBB intact. [7] The practical result of this partnership is profound: patients can take lower doses of L-DOPA, experience fewer peripheral side effects like vomiting, and achieve better symptomatic control because more of the active drug reaches the central nervous system. [4][6] It is difficult to overstate the clinical necessity of this combination; administering Levodopa without Carbidopa (or its analogue, Benserazide, used outside the US) is largely impractical for long-term Parkinson’s management due to the resulting systemic side effects. [7]
# Symptom Improvement
The relief provided by the L-DOPA/Carbidopa combination targets the most debilitating aspects of Parkinsonian movement. [6] Patients often report significant improvements in:
- Bradykinesia (Slowness): The difficulty initiating and executing movement is often the most dramatically improved symptom. [6]
- Rigidity (Stiffness): Muscle rigidity, which contributes to a stooped posture and painful cramping, typically lessens considerably. [6]
- Tremor: While tremor can respond, it is sometimes less reliably controlled by L-DOPA than bradykinesia or rigidity. [6]
The effectiveness can be so pronounced that it serves as a diagnostic tool. If a patient suspected of having Parkinson’s disease shows a clear, positive response to L-DOPA, it strongly supports the diagnosis, especially in cases of young-onset or juvenile parkinsonism. [5]

# Dose Timing
While the immediate effect of a dose is to provide symptom relief, the experience of taking these medications is not static over time. One subtle aspect that influences daily life is the relationship between drug absorption and stomach contents. Certain foods, particularly high-protein meals, can actually compete with L-DOPA for absorption in the small intestine. [4] This competition can slow down the rate at which the medication enters the bloodstream, delaying the onset of symptom control when it is needed most. Therefore, timing medication around meals often becomes a finely tuned part of a person’s daily routine, adjusting dosages to be taken an hour before or two hours after eating to ensure reliable uptake. [4]
# Long-Term Challenges
Although L-DOPA is the gold standard, its use over many years, as is necessary for chronic Parkinson's management, often introduces new complications. [10] The brain's ability to process and utilize the drug changes, leading to what are known as motor fluctuations. [4][10]
These fluctuations involve periods where the medication is working well—the "on" time—followed by periods where the effect wears off too soon, and symptoms return before the next dose—the "off" time. [7][10] This can make a person's mobility unpredictable throughout the day.
A more complex complication that can arise from prolonged treatment is dyskinesia. [4][7] Dyskinesias are involuntary, erratic, writhing movements that are often opposite to the slowness of Parkinson's. [4] They are thought to be a long-term consequence of the brain adapting to fluctuating dopamine stimulation. [7] Managing dyskinesia often requires complex adjustments to the L-DOPA regimen, sometimes involving switching to different formulations or adding adjunctive therapies. [4]

# Other Applications
Beyond its central role in Parkinson's disease, L-DOPA has been noted for its use in treating other conditions, though usually in different contexts or formulations. [1][5] One notable secondary application is in the management of Restless Legs Syndrome (RLS). [1][5] RLS is characterized by an uncomfortable, irresistible urge to move the legs, often worse at night or during periods of rest. [5] While the mechanism is related to dopamine pathways, the treatment strategy for RLS may differ from that used for Parkinson's. [1]
Furthermore, as mentioned previously, L-DOPA can be used specifically to diagnose certain types of parkinsonism, particularly primary juvenile parkinsonism, by observing the dramatic positive response to the drug. [5]
# Delivery Methods
To help manage the on/off fluctuations and the challenges of absorption, L-DOPA/Carbidopa is made available in several specialized formulations. [4] Patients and their neurologists select the appropriate type based on symptom severity and fluctuation profile:
- Immediate-Release Tablets: These work quickly but have a shorter duration of action, which can contribute to wearing-off periods. [4]
- Extended-Release Tablets: Designed to dissolve slowly, these aim to provide more consistent drug levels over a longer period, potentially smoothing out the peaks and troughs. [4]
- Immediate-Release Plus Carbidopa: This standard combination is the baseline for many patients. [4]
- Combination with Entacapone: In some formulations, L-DOPA/Carbidopa is combined with Entacapone, which acts as a peripheral COMT inhibitor, further blocking the peripheral breakdown of L-DOPA and extending its effective duration. [4]
The choice among these forms often evolves over the course of the disease. An initial reliance on immediate-release doses might transition to extended-release formulas or the introduction of supplementary drugs as the underlying disease progresses and the patient's dopamine requirements become less stable. [10] Understanding the precise formulation and how it interacts with the body’s absorption kinetics is key to maximizing the therapeutic window—that time after taking a dose when the medication is working optimally—while minimizing the disruptive impact of off-periods and dyskinesia. [4]
Related Questions
#Citations
Levodopa (L-Dopa) - StatPearls - NCBI Bookshelf - NIH
Levodopa and Carbidopa: MedlinePlus Drug Information
Levodopa: Uses, Interactions, Mechanism of Action | DrugBank
Carbidopa and levodopa (oral route) - Side effects & dosage
L-DOPA - Wikipedia
Levodopa - Parkinson's Foundation
Levodopa & Carbidopa for Parkinson's: The Good, the Bad, the Truth
L-DOPA - an overview | ScienceDirect Topics
Parkinson's Disease Medications: What They Are & Side Effects
Parkinson's disease - Treatment - NHS