What causes Romanus lesion?
The appearance of a Romanus lesion in the spine signals a very specific and significant underlying process, almost always pointing directly toward Ankylosing Spondylitis (AS). [1][4] These lesions are not standalone conditions but rather a hallmark sign of chronic inflammation within the vertebral column associated with this systemic rheumatic disease. [3][5] To understand what causes a Romanus lesion, one must first understand the relentless inflammatory cascade that characterizes AS itself. [9] The key mechanism driving these bony changes is enthesitis—inflammation where tendons, ligaments, or joint capsules attach to bone—which, in the spine, targets the vertebral margins. [1][6]
# Inflammatory Root
Ankylosing Spondylitis is categorized as a chronic, progressive inflammatory arthritis that predominantly affects the axial skeleton, meaning the spine and the sacroiliac joints. [5][9] It is an autoimmune condition where the body's immune system mistakenly attacks healthy tissue, leading to persistent inflammation. [3] The resulting damage in AS follows a predictable, though destructive, sequence along the spinal column. [4]
The initiating event for a Romanus lesion is this localized inflammation, or enthesitis, occurring precisely at the junction where the tough, fibrous outer layer of the intervertebral disc, known as the annulus fibrosus, inserts into the adjacent bone of the vertebral body. [1][6] This spot is a vulnerable interface where mechanical stress meets immunological activity, making it a prime target for the disease process. [3]
When the inflammation is active at this attachment point, the body initiates a destructive, localized response. The initial effect on the bone is erosion. [1][6] In the context of imaging, this erosion presents as small defects or indentations in the subchondral bone plate right at the anterior (front) edge of the vertebral body, adjacent to the disc space. [1][6] This is the nascent stage of the Romanus lesion.
It is interesting to consider that while the primary event is inflammatory erosion, the body attempts to repair this damage almost immediately, leading to the next crucial stage. [1] This inherent drive toward repair, even in the face of ongoing chronic disease, is what ultimately defines the lesion's progression.
# Pathological Sequence
The development of a Romanus lesion is a clear, stage-dependent phenomenon in the spinal progression of AS, moving from pure inflammation to structural change. [1][4]
The process unfolds in distinct steps:
- Inflammation (Active Enthesitis): The immune response targets the enthesis at the anterior vertebral rim. [3][6]
- Erosion: Localized bone resorption occurs, creating the initial "lesion"—a marginal defect visible on imaging. [1]
- Reactive Sclerosis: As a reparative mechanism against the defect, bone-forming cells (osteoblasts) lay down new, dense bone tissue in the affected area. [1][6] This healing response results in sclerosis, which appears as a denser, whiter area on radiographic images.
A key feature distinguishing a Romanus lesion from other types of spinal injury or infection is its location and its dual nature: it simultaneously shows signs of damage (erosion) and over-repair (sclerosis). [1] While the erosion itself is an initial manifestation, the sclerosis is often what makes the lesion definitively identifiable in standard X-rays or CT scans. [6] The severity of the sclerosis is often indicative of the chronicity or activity level of the underlying inflammatory disease in that segment.

# Imaging Presentation
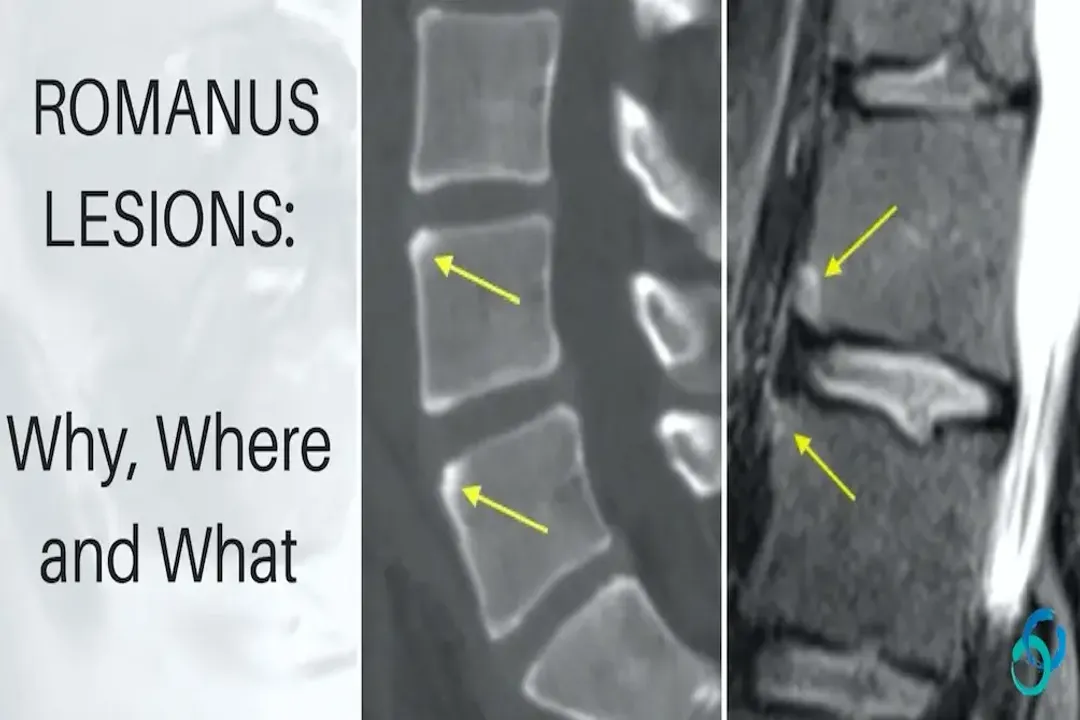
Radiologically, Romanus lesions are most frequently found in the lower thoracic and upper lumbar spine. [1][4] They appear as small, distinct defects or patches of increased density (sclerosis) located precisely at the corners or margins of the vertebral bodies adjacent to the intervertebral discs. [6]
When using Magnetic Resonance Imaging (MRI), which is more sensitive to early inflammation, an active Romanus lesion may show signs of edema (fluid accumulation) in the adjacent bone marrow, which reflects the ongoing inflammatory process, sometimes referred to as vertebral osteitis. [6] This early MRI signal is critical because it detects the cause (inflammation) before the chronic result (sclerosis) becomes overwhelming. A Romanus lesion, therefore, represents the point where the spinal inflammation has begun to leave a visible, chronic radiographic scar. [1]
Considering imaging protocols, a general insight emerges regarding the earliest detection: relying solely on plain X-rays misses the active inflammatory component. If a patient with clinical symptoms suggestive of AS receives an X-ray showing no Romanus lesions, an MRI might reveal the subclinical, active enthesitis occurring at the disc-bone interface, offering an opportunity for earlier intervention to halt the erosive cycle before significant sclerosis sets in.
# Progression and Differentiation
The Romanus lesion is not the final stage of spinal involvement in AS; rather, it serves as a precursor to more severe structural changes. As the chronic inflammation continues unabated over many years, these lesions evolve. [1][4]
# Lesion Maturation
The initial Romanus lesion, characterized by marginal erosion and mild sclerosis, matures into what is termed an Andersson lesion. [1][6] Andersson lesions are essentially established or "healed" Romanus lesions that have undergone extensive reactive bone formation. [6]
The difference is quantitative and qualitative:
- Romanus Lesion: Smaller, often involving only one corner margin, less pronounced sclerosis.
- Andersson Lesion: Larger, more substantial sclerosis, often appearing as prominent, dense lesions at the vertebral corners. [4][6]
The development of Andersson lesions signifies a long-standing, established pattern of disease activity in that spinal segment. [1] In rare instances, the intense reactive bone formation can bridge the disc space entirely, leading to the characteristic syndesmophytes seen in advanced AS. [1][4] Therefore, identifying a Romanus lesion is an early warning sign that the process leading to spinal fusion—the infamous "bamboo spine"—has initiated at that vertebral level. [4][9]

# Etiological Comparison
It is helpful to compare Romanus lesions to other types of vertebral bone damage to solidify understanding of their specific cause. Many conditions can cause bone erosion or sclerosis in the spine, such as infection (osteomyelitis) or metastatic disease, but the location and pattern are key differentiators. [1]
For instance, in discitis or typical vertebral osteomyelitis, the primary destruction is centered within the disc space and the adjacent vertebral endplates symmetrically, rather than strictly marginal at the bone-disc interface as seen in Romanus lesions. [1] Similarly, degenerative changes cause different patterns of endplate irregularity and osteophyte formation that lack the distinct erosive focus followed by intense marginal sclerosis characteristic of AS. [3] The cause is rooted in the systemic inflammatory nature of AS attacking a specific biomechanical junction, not a localized infection or standard mechanical wear-and-tear.
If we were to assign a crude "Activity Score" based purely on imaging findings related to the Romanus lesion sequence, we might establish a rudimentary scale for educational purposes:
| Stage | Primary Finding | Underlying Process Implied |
|---|---|---|
| Stage 0 | Normal imaging/Mild MRI edema | Active Enthesitis (Pre-lesion) |
| Stage 1 | Minor marginal erosion/sclerosis | Early Enthesitis/Repair Cycle |
| Stage 2 | Prominent Romanus Lesion | Established, persistent inflammatory attack |
| Stage 3 | Advanced sclerosis (Andersson Lesion) | Long-standing, potentially quiescent repair |
This progression underscores that the cause is the disease activity itself. Effective management of AS is aimed squarely at interrupting the transition from Stage 1 to Stage 3 by controlling the underlying inflammation. [3][5] Successfully managing the systemic disease activity is, by extension, the only way to prevent the formation of new Romanus lesions and allow existing ones to stabilize or regress slightly, though significant established sclerosis may remain permanent. [5] The presence of these lesions confirms the diagnosis of AS when clinical suspicion is present and helps track disease burden along the spine. [9]
Related Questions
#Citations
Romanus lesion - Wikipedia
THE ROMANUS LESION: WHY, WHERE AND WHAT - Radedasia
Discovertebral (Andersson) lesions of the spine in ankylosing ...
Ankylosing Spondylitis - Radsource
The fatty Romanus lesion: a non-inflammatory spinal MRI lesion ...
Andersson and Romanus lesions | Radiology Case | Radiopaedia.org
Disco-vertebral destructive lesions (So-called Andersson Lesions ...
The fatty Romanus lesion: a non-inflammatory spinal MRI lesion ...
Ankylosing Spondylitis - Spine - Orthobullets