What is the antidote for paraquat?
Paraquat poisoning represents one of the most significant challenges in toxicology due to its rapid systemic uptake and the resulting multi-organ damage it causes, particularly to the lungs and kidneys. When facing exposure, the immediate and often desperate question revolves around finding a specific chemical agent—a true antidote—that can neutralize the toxin inside the body. However, the reality of managing paraquat intoxication is markedly different from many other common poisonings because a universally effective, direct chemical antidote does not currently exist.
# Toxicity Mechanism
Understanding why an antidote is elusive requires grasping how paraquat exerts its devastating effects. Paraquat, chemically known as paraquat dichloride, is a highly toxic quaternary ammonium herbicide. Once absorbed, often rapidly through the gastrointestinal tract after ingestion, it is taken up selectively by type I and type II pneumocytes in the lungs, which are crucial for its toxicity.
The mechanism involves redox cycling. Inside the cells, paraquat accepts an electron to form a paraquat radical. This radical then reacts with molecular oxygen, regenerating the original paraquat molecule and simultaneously creating damaging reactive oxygen species (ROS), such as superoxide radicals. This process repeats itself continuously, overwhelming the cell’s natural antioxidant defenses and leading to massive oxidative stress, lipid peroxidation, and eventually cell death. This relentless cycle is what makes the poison so lethal and difficult to stop once established.
# Absence Specific Agent
The medical community acknowledges that there is no single agent that can reliably reverse the cellular damage caused by paraquat once it has entered the bloodstream and begun its toxic cycle. Unlike poisonings where an antagonist drug exists—such as naloxone for opioids or atropine for organophosphates—paraquat treatment relies instead on a multi-pronged approach centered on prevention of further absorption and supportive care for failing organs. The lack of an antidote means that successful outcomes hinge almost entirely on the speed and efficacy of initial decontamination measures.

# Decontamination First Steps
The very first priority following suspected ingestion is to prevent any more of the poison from entering the bloodstream. If the patient is conscious and able to swallow, immediate administration of an inert adsorbent substance is initiated right away. For patients who have just ingested the material, thorough washing of the skin and eyes is essential to prevent dermal absorption, although ingestion is the primary route of severe poisoning.
While gastric emptying procedures like induced vomiting are generally discouraged in clinical settings for many toxins due to aspiration risk, specific guidelines sometimes call for activated charcoal or adsorbents administered quickly, provided the patient is alert.
# Adsorption Binders
Since stopping the redox cycle inside the body is not possible with a specific drug, the focus shifts to binding the paraquat in the gut to prevent its absorption. The efficacy of this strategy is critically time-dependent. The speed at which paraquat is absorbed from the gastrointestinal tract means that successful binding relies on administration within minutes of ingestion, highlighting a severe challenge for pre-hospital care or in regions where immediate medical access is delayed. If the poison has already begun to be absorbed, the binders will have limited effect on the systemic toxicity that is already underway.
Effective binding agents utilized in the acute phase include:
- Fuller's Earth (Bentonite): This is often cited as the preferred agent due to its high binding capacity for paraquat.
- Activated Charcoal: This is another adsorbent commonly used in poison management, although Fuller's Earth is sometimes favored specifically for paraquat due to superior binding capability.
In some treatment protocols, a large amount of the adsorbent, often mixed with a cathartic like sorbitol to speed transit through the gut, is administered. This is a mechanical intervention intended to physically trap the herbicide molecules, preventing them from passing through the intestinal wall into circulation.
# Supportive Management
Once absorption has occurred or while binding agents are being administered, the medical management transitions entirely to intensive supportive care aimed at minimizing the consequences of organ damage. This phase requires admission to an intensive care unit (ICU) setting.
# Pulmonary Care
The lungs are often the final target organ, leading to pulmonary fibrosis and respiratory failure, which is a major cause of death. Supportive respiratory care might involve supplemental oxygen. If respiratory failure is advanced, mechanical ventilation may be necessary, though decisions must be carefully weighed against the prognosis, as severe lung damage can make ventilation futile.
# Renal Replacement Therapy
Paraquat is rapidly excreted by the kidneys, and high concentrations can cause acute kidney injury. Maintaining fluid balance and monitoring kidney function are paramount. In cases of significant renal failure, continuous renal replacement therapy (like hemodialysis) may be employed, not only to manage fluid and electrolyte imbalances but also potentially to remove some of the circulating paraquat, although its effectiveness in removing already distributed toxin is limited.
# General Care
Systemic support includes monitoring and correcting electrolyte disturbances, managing circulatory shock if present, and treating any secondary infections that may arise due to the patient’s critical state. Experimental treatments, such as the use of glucocorticoids or cyclophosphamide, have been investigated to try and mitigate the later fibrotic phase of lung injury, but evidence supporting their routine use remains inconclusive.
# Prognosis Factors
Predicting the outcome of paraquat poisoning is strongly linked to measurable factors available early in the clinical course. The concentration of paraquat ingested and the time elapsed between ingestion and the start of effective treatment are the most significant determinants of survival.
The fatality risk dramatically increases depending on the concentration ingested. While commercial products typically contain active ingredients around $27.7%$, ingestion of even relatively small quantities of concentrated solutions is often fatal. A generally accepted clinical indicator is that ingestion of more than 5 mL of a $20%$ paraquat solution is associated with a high mortality risk. Furthermore, if plasma concentrations remain above a certain threshold hours after exposure, the prognosis darkens considerably.
Considering the potency, it is useful to note that agricultural formulations are designed for high efficacy, meaning even small volumes consumed accidentally or intentionally carry a massive toxic load relative to the human body weight. This high toxicity profile is why preventive measures are prioritized globally.

# Prevention Measures
Given the near-intractability of treatment once systemic absorption is complete, controlling access to the herbicide is a critical public health intervention. Regulations surrounding paraquat use vary significantly worldwide. Several jurisdictions have moved toward banning or severely restricting its use due to the high incidence of intentional self-poisoning cases. For instance, while it remains registered in some areas, the EPA monitors its use closely in the United States. In many other countries, regulations mandate stricter controls, often limiting sales only to certified applicators or banning formulations above a certain concentration threshold. This regulatory approach acknowledges that the most effective management strategy remains preventing the exposure in the first place.
Related Questions
#Citations
Medical management of paraquat ingestion - PMC - PubMed Central
Paraquat Poisoning: Symptoms & Treatment - Cleveland Clinic
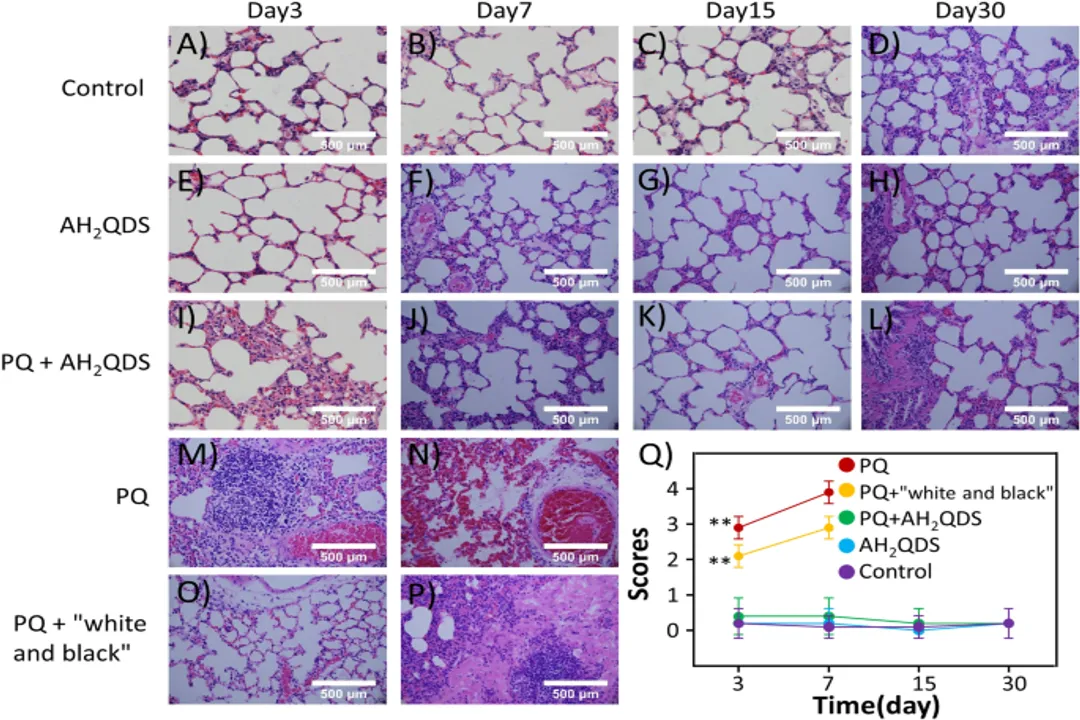
Anthrahydroquinone-2-6-disulfonate: Antidote for paraquat poisoning
Paraquat | Chemical Emergencies - CDC
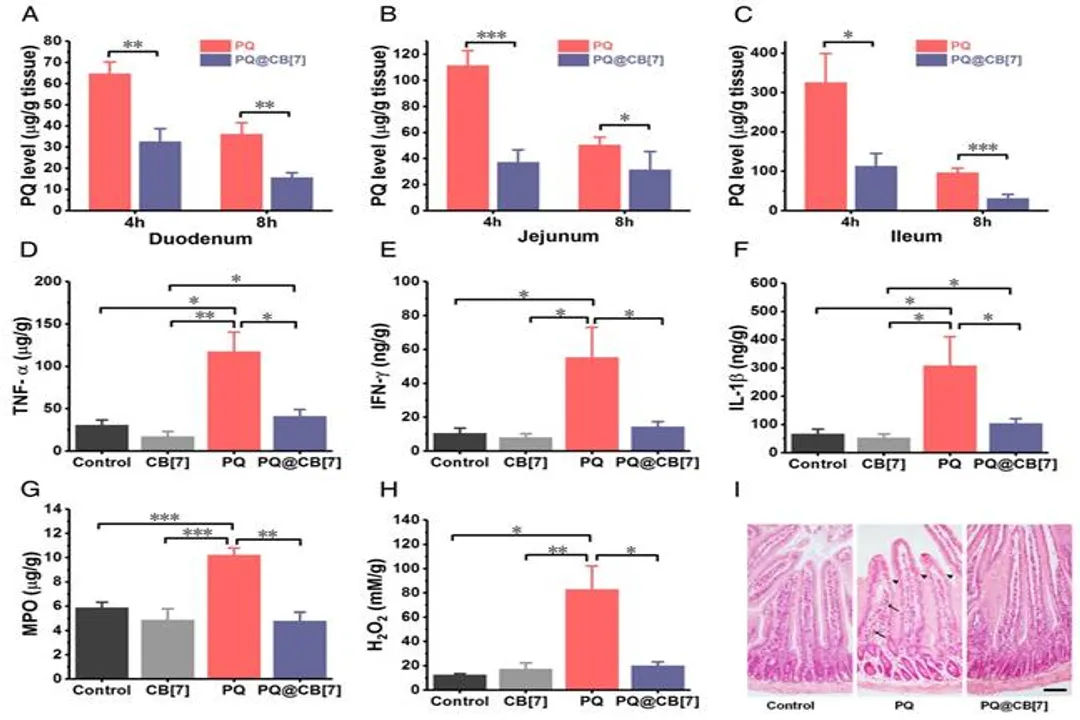
A Synthetic Receptor as a Specific Antidote for Paraquat Poisoning
Delaware Health Alert Network #16
Paraquat Dichloride | US EPA
An effective antidote for paraquat poisonings: The treatment with ...
Paraquat Poisoning: Gramoxone, Toxicity, and Side Effects
[PDF] Paraquat Poisoning: One Sip Can Kill - OHSU