What is dicrocoeliasis?
The presence of tiny parasitic flatworms, specifically Dicrocoelium dendriticum, within the bile ducts of mammals, including humans, leads to a condition known as dicrocoeliasis. [1][6] While often associated with livestock, this trematode infection can sporadically affect people, typically through the accidental ingestion of the intermediate host. [2][4] This infection is generally considered rare in humans compared to other helminthic diseases, but understanding its mechanism, spread, and potential for causing symptoms is important, especially in endemic rural areas. [5][7] The parasite itself is commonly referred to as the lancet liver fluke due to its shape. [6]
# The Lancet Fluke
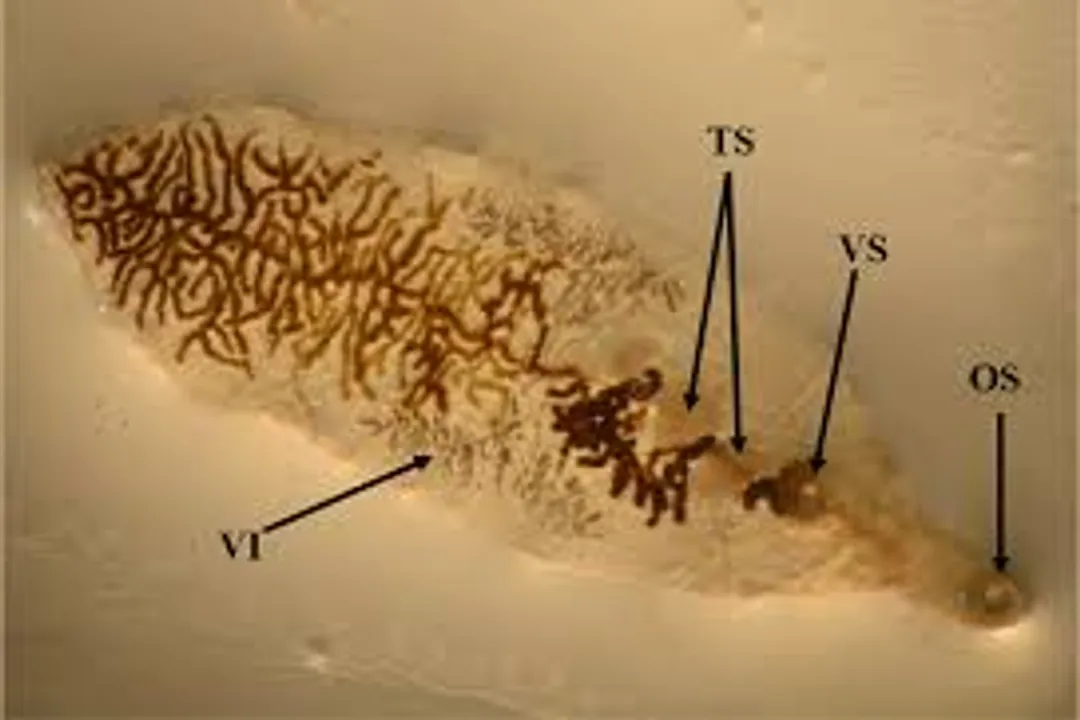
Dicrocoelium dendriticum belongs to the phylum Platyhelminthes and the class Trematoda. [6] Adult flukes residing in the host's biliary system are small, flat, and lance-shaped, measuring about 6 to 10 millimeters in length and 1.5 to 2 millimeters in width. [6][1] They possess two suckers, an oral sucker and a ventral sucker, which aid in their attachment within the bile ducts. [6] These worms are hermaphroditic, meaning each individual possesses both male and female reproductive organs, allowing them to self-fertilize or cross-fertilize. [6] The eggs they produce are small, thin-shelled, and operculated (meaning they have a lid), which is a characteristic feature enabling them to exit the host via feces. [6][2]
The diagnosis of dicrocoeliasis relies heavily on identifying these characteristic eggs in the patient's stool samples. [2][5] The morphology of the eggs—ellipsoidal with a distinct operculum at one end and often a small knob or mucilaginous mass at the other—is key for differentiation from other liver flukes, such as Fasciola hepatica. [6][7]
# Complex Transmission Cycle
Dicrocoeliasis is characterized by a peculiar and complex life cycle involving three different hosts: a terrestrial snail (first intermediate host), an ant (second intermediate host), and a final vertebrate host, which can be a grazing animal or, less commonly, a human. [2][6] This specific requirement for a terrestrial insect, the ant, to act as the second host is a defining feature that differentiates it epidemiologically from many other trematode infections that utilize aquatic snails or crustaceans. [6]
The cycle begins when the operculated eggs are passed in the feces of an infected definitive host, such as a sheep, goat, or cow. [2] If these eggs land in a suitable environment, they must be ingested by the first intermediate host, a terrestrial snail, often belonging to the genera Cochlicopa, Zebrina, or Helicella. [6] Inside the snail, the miracidium hatches and undergoes asexual reproduction, developing through sporocyst and redia stages into cercariae. [6]
This is where the cycle takes its unusual turn. Instead of being released into water, the cercariae migrate out of the snail and actively penetrate the body cavity of a specific ant species, commonly Formica fusca. [6] Within the ant, the parasites encyst as metacercariae, which is the infective stage for the final host. [2][6] For the metacercariae to develop fully and become infective, the ant must exhibit a behavioral alteration; the parasites manipulate the ant's central nervous system to cause it to climb to the tip of a blade of grass or a leaf, often in the morning dew. [6] This "summiting" behavior, essentially an advertisement, makes the infected ant much more likely to be accidentally ingested by the final grazing host. [6]
Ingestion of the infected ant by the definitive host—such as cattle, sheep, pigs, goats, or humans—completes the cycle. [2][6] Once swallowed, the metacercariae excyst in the duodenum, penetrate the intestinal wall, migrate through the peritoneal cavity, and eventually reach the liver via the portal veins, ultimately settling and maturing in the bile ducts. [6][1] The prepatent period, the time from infection until eggs appear in the feces, can range from 7 to 16 weeks. [6]
It is worth noting the contrast in transmission ecology here: while common relatives like Fasciola rely on aquatic snails and free-swimming stages necessitating water contact for infection, Dicrocoelium is intrinsically linked to terrestrial grazing habits and the specific manipulation of soil-dwelling insects. [6] This ecological niche explains why infection risk is highest in pastoral settings where livestock graze. [7]
# Geographic Spread and Human Risk
Dicrocoeliasis has a wide, though often focal, distribution across the globe, reflecting the presence of susceptible definitive hosts, the correct snail species, and the specific Formica ant species. [8] Historically, the disease has been reported in regions encompassing Southern and Eastern Europe, the Middle East, North Africa, Asia, and the Americas. [8][6] Areas with warm, temperate climates and appropriate grazing land are considered most prone to endemicity. [8]
While domestic ruminants like sheep and goats are the principal hosts and the main source of environmental contamination, human infection occurs primarily due to accidental ingestion of the second intermediate host, the infected ant. [2][6] This usually happens when people consume untreated food or water in endemic regions, or perhaps by accidentally ingesting ants found on wild berries or vegetables collected from the ground. [4][7] The actual prevalence of human cases is believed to be much lower than the actual infection rate in domestic animals, partly because human infections often go undiagnosed or are asymptomatic. [5]
When considering risk profiles, individuals working closely with livestock or those living in rural areas with known cattle infection rates should be particularly aware of the potential for low-level chronic exposure, even if overt clinical disease is uncommon. [7] A fascinating regional observation, though not universally documented, suggests that while the parasite is widespread, high-intensity outbreaks in human populations are rare, perhaps due to variations in human dietary habits that decrease the frequency of ant ingestion compared to ruminants. [7]
# Clinical Picture
The clinical presentation of dicrocoeliasis in humans is highly variable, ranging from entirely asymptomatic infections to severe liver pathology, largely depending on the worm burden and the duration of the infection. [4][5] In many instances, especially with light infections, individuals remain completely asymptomatic, and the condition is discovered only incidentally during routine fecal examination for other gastrointestinal issues. [5]
When symptoms do manifest, they are typically related to the physical presence of the worms obstructing the bile ducts and the subsequent inflammation and pathological changes in the liver and surrounding tissues. [1] Common complaints mimic other hepatobiliary disorders and include:
- Abdominal pain, often localized in the upper right quadrant. [4][5]
- Nausea and vomiting. [4]
- Fever. [5]
- Loss of appetite or weight loss. [1]
- Diarrhea. [5]
In cases of heavy, chronic infection, more serious complications can arise due to long-term irritation and obstruction of the biliary tree. [1] Pathologically, the flukes cause inflammation of the bile ducts (cholangitis) and periductal fibrosis. [1][5] Prolonged inflammation can lead to changes in the bile duct epithelium. [1] Severe, long-standing infestations have been linked to rarer, more significant complications, such as biliary obstruction, the formation of gallstones (cholelithiasis), or even, in some documented but very infrequent cases, cholangiocarcinoma (cancer of the bile ducts). [1][5]
Unlike the acute systemic illness caused by Fasciola hepatica (which involves significant tissue migration), the pathology in dicrocoeliasis is generally more localized to the biliary tract once the flukes reach the liver, as D. dendriticum tends to remain confined within the ducts rather than migrating extensively into the liver parenchyma. [1] This confined nature influences the type of symptoms seen.
# Identifying and Managing Infection
Confirming a diagnosis of dicrocoeliasis usually requires laboratory confirmation of the parasite or its products. [2]
# Diagnostic Techniques
The cornerstone of diagnosis remains fecal examination. [5] Stool samples are analyzed, often employing concentration techniques to increase the likelihood of detecting the characteristic small, thin-shelled, operculated eggs. [2][7] Since eggs can be shed intermittently, multiple stool samples collected on different days might be necessary for a definitive diagnosis, especially if clinical suspicion is high despite negative initial tests. [7]
Imaging techniques are sometimes employed to assess the extent of damage to the biliary system, particularly if the patient presents with obstructive symptoms. [4] Ultrasound, CT scans, or magnetic resonance cholangiopancreatography (MRCP) might reveal evidence of biliary dilation or ductal wall thickening, though these findings are not specific to dicrocoeliasis alone. [1]
For a specialized insight into diagnosis, consider that while egg morphology is standard, molecular techniques like PCR, though not standard clinical practice yet, offer the potential for highly sensitive and specific identification, especially in mixed infections or when eggs are scarce. [3] Researchers have worked on developing such techniques, which could one day supplement traditional microscopy, particularly in reference laboratories. [3]
# Treatment Protocols
When treatment is indicated, usually due to symptomatic infection or high worm burden, the preferred agents are generally those effective against other fluke infections. [5] The drug of choice for treating Dicrocoeliasis is Praziquantel. [5][2]
Praziquantel is an anthelmintic drug that paralyzes the parasite, leading to its disintegration and expulsion from the body, often within the bile ducts where it is then passed out. [2] Dosing regimens typically mirror those used for other trematodes, but specific protocols should always be determined by a healthcare provider based on the patient's weight and the severity of the infection. [5] Alternative agents like albendazole or mebendazole have been mentioned in the context of treating helminths, but Praziquantel is generally the recommended treatment for Dicrocoelium. [5]
Following successful treatment, follow-up stool examinations are crucial to confirm the clearance of the infection, as eggs may persist for a period even after the worms have been eliminated. [2]
# Proactive Avoidance Strategies
Because treatment success depends on accurate diagnosis and the infection is fundamentally acquired through environmental exposure, prevention stands as the most effective public health strategy against dicrocoeliasis. [2] Control measures center on interrupting the life cycle at several key points.
In agricultural settings, the management of intermediate hosts is paramount. Controlling the snail population in pastures, though difficult due to their terrestrial nature, can reduce transmission to livestock. [6] Furthermore, treating infected grazing animals, particularly sheep and goats, is vital to reduce the environmental load of eggs being shed into the soil. [2]
For human protection, the necessary measures focus directly on the ingestion pathway:
- Hygiene: Emphasizing rigorous handwashing, especially after working outdoors or before handling food. [4]
- Food Preparation: Avoiding the consumption of wild berries, leafy greens, or herbs collected directly from the ground or low-growing vegetation in endemic areas unless they are thoroughly washed. [4][7] Since the infective stage is the ant itself, anything that might harbor ants coming from the soil poses a theoretical risk.
- Water Safety: Ensuring drinking water is from a reliably treated or uncontaminated source, although the primary risk route is ingestion via ants, not waterborne cysts. [2]
An actionable tip for residents or travelers in high-risk pastoral zones involves a simple food preparation checklist: Any fresh, uncooked produce taken from the immediate ground level should be subjected to a three-stage cleaning process—a quick rinse to remove surface debris, followed by a thorough soak in clean water (potentially with a small amount of disinfectant like diluted vinegar or iodine if tap water quality is questionable), and a final rinse under running water. [7] This layered approach accounts for both surface contaminants and the possibility of small, hidden insects being present on the foliage. Given that the parasite manipulates the ant to perch high, targeting low-lying vegetation for collection is only a partial mitigation; diligent washing addresses the accidental ingestion risk across various scenarios. [6] The goal is to minimize the chance that a single, infective ant is consumed along with the edible plant matter.
# Current Research and Future Context
While dicrocoeliasis remains a relatively minor human health concern globally, its presence in veterinary medicine is more significant, often leading to economic losses in animal husbandry due to decreased productivity and compromised animal health in endemic regions. [1][8] Ongoing scientific efforts focus on better understanding the precise ecological requirements for the parasite's survival and transmission, which may lead to more targeted control strategies. [7]
For instance, research continues into the specific biochemical interactions that cause the ant to climb the vegetation, as understanding this manipulation might reveal vulnerabilities in the parasite's developmental process. [6] Moreover, the fact that human cases are sporadic and often mild suggests that our general lifestyle, which involves less direct grazing contact than ruminants, offers a natural, albeit incomplete, protective barrier. [5] However, the potential for severe, chronic biliary disease in infected individuals underscores the need for vigilance where the parasite cycle is active. [1] The overall picture confirms dicrocoeliasis as a zoonosis strongly linked to specific agricultural practices and local terrestrial ecosystems. [8]
Related Questions
#Citations
Dicrocoeliasis - an overview | ScienceDirect Topics
DPDx - Dicrocoeliasis - CDC
Human dicrocoeliasis presenting as a subcutaneous mass - PMC
What Is Dicrocoeliasis? - iCliniq
Dicrocoeliasis - DoveMed
Dicrocoelium dendriticum - Wikipedia
[PDF] Dicrocoelium dendriticum: a true infection? - InfezMed
Dicrocoeliasis worldwide distribution - GIDEON Informatics
Dicrocoelium dendriticum: a true infection? - PubMed